
Is a Flexion MRI Needed After a Normal Supine Scan?
Being told that an MRI is normal is supposed to be reassuring, but for many patients it is anything but. When the pain is real, when the symptoms are consistent and disabling, and when the MRI that was meant to explain everything comes back showing nothing of significance, the result creates a different kind of problem. The patient is left without a diagnosis, without a treatment plan, and sometimes with the implicit suggestion that the pain is not structural, or worse, not real.
What many of these patients are experiencing is not a mystery. It is a measurement problem. The supine MRI captures the spine in the one position where most structural problems are at their least apparent: lying flat, offloaded from gravity, in a neutral position. For a significant subset of spinal conditions, particularly those involving instability, ligamentous laxity, or load-dependent compression, this is precisely the position that produces the fewest abnormal findings. The problem is real. The scan was simply taken in the wrong position.
Quick Answer: A flexion MRI is frequently warranted after a normal supine scan when the patient has significant symptoms that are clearly worsened by specific positions, particularly forward bending, and when the clinical presentation suggests instability or dynamic compression. A normal supine MRI does not rule out structural spine pathology. It rules out structural abnormality in the supine position only.
What a Normal Supine MRI Actually Tells You
A supine MRI is an excellent tool for detecting many types of spinal pathology. Large disc herniations, significant tumours, fractures, osteomyelitis, and other conditions with a strong structural signature that is present regardless of position show up reliably on supine imaging. For these categories of pathology, a normal supine scan is genuinely reassuring.
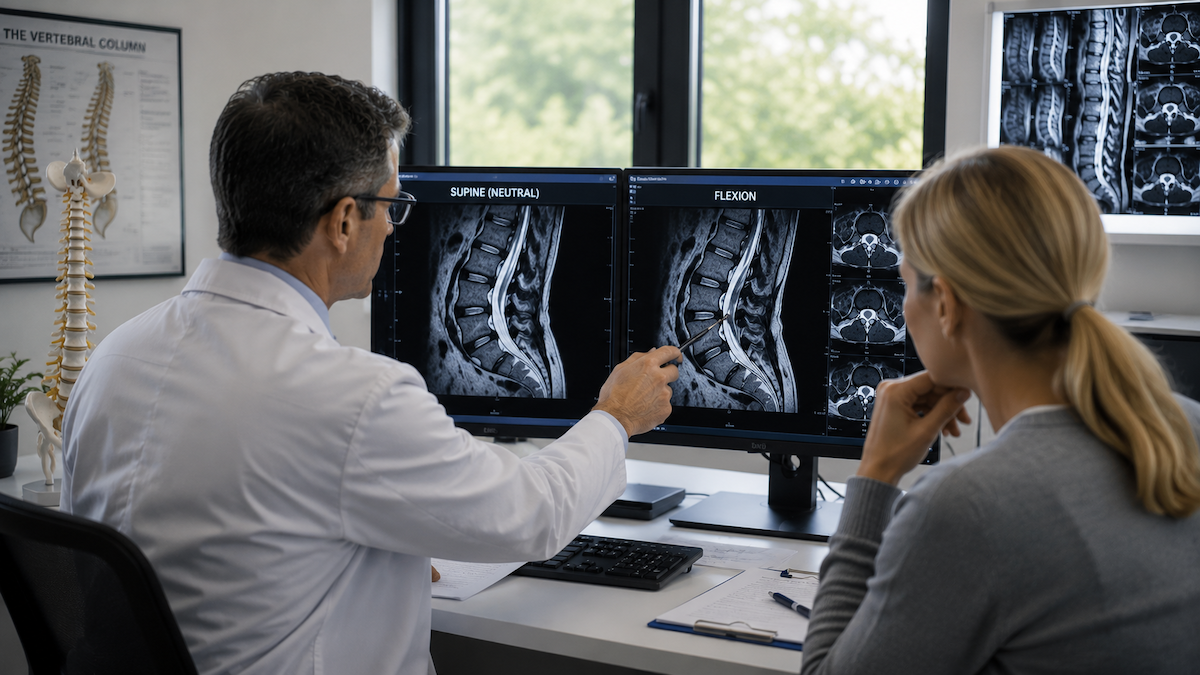
The categories it does not reliably detect are those where pathology is position-dependent. Ligamentous instability that only becomes apparent under load. Foraminal stenosis that is present when the spine is extended but absent when the patient lies down. Segmental motion abnormalities that require the spine to flex or extend to become visible. Dynamic disc bulging that increases substantially in the sitting or flexed position compared to lying flat.
There is substantial clinical evidence that traditional MRI routinely misses positional pathology of this kind, which is why patients with consistently normal supine imaging and persistently symptomatic spines deserve further investigation rather than reassurance that nothing is wrong.
When a Flexion MRI Is the Logical Next Step
The clearest indication for a flexion MRI after a normal supine scan is a symptom pattern that is consistently and specifically worse with forward bending or activity. A patient who has no pain lying down but develops significant leg pain, back pain, or neurological symptoms within minutes of standing up, walking, or bending forward is describing a load-dependent or positional problem that a supine scan cannot measure.
Patients who have previously had spinal surgery and develop recurrent symptoms are another group where flexion and extension imaging adds significant value. Post-surgical instability at adjacent levels, which is a well-recognised complication of spinal fusion, may only be apparent under dynamic conditions. A repeat supine scan in these patients often shows the original fusion intact and may miss the adjacent segment problem entirely.
The specific conditions that most consistently benefit from flexion and extension imaging is critical for evaluating include spondylolisthesis where the degree of slip changes with position, cervical and lumbar instability, and spinal stenosis that is clinically significant under load but minimal at rest.
What Flexion Imaging Finds That Supine Scans Miss
In the lumbar spine, lumbar flexion MRI uncovers hidden compression of the thecal sac and nerve roots that was absent or minimal in the supine study, particularly when ligamentum flavum is thickened or when disc pathology worsens in the flexed position.
The most striking examples are patients with neurogenic claudication, the pattern of leg symptoms that develops with walking and standing and resolves with sitting or forward bending. The mechanism is dynamic narrowing of the spinal canal under extension load. A supine scan in neutral position may show only modest stenosis while the flexed or axially loaded scan demonstrates the severe narrowing that produces the symptoms.
Beyond compression, positional MRI reveals hidden spine issues such as translational instability where one vertebral body moves forward or backward on the one below it during flexion, creating a shear force on the disc and ligamentous structures that is the direct source of the patient's pain.
The principle that supine imaging is not always sufficient is not a criticism of conventional MRI technology. It is a recognition that imaging a structure in a single static position cannot capture the full range of its behaviour, particularly for a structure as mechanically complex and load-sensitive as the human spine.
The Nerve Compression Dimension
One of the most clinically important advantages of positional MRI is that nerve compression is better detected positionally in patients whose symptoms are specifically neurological, because the degree of foraminal and canal compromise that a nerve is actually experiencing when the patient is symptomatic may be dramatically different from what the supine scan suggests.
Foraminal dimensions change substantially between supine and upright positions, and change further with flexion and extension. In many patients with radiculopathy, the foraminal narrowing responsible for the nerve root compression is only measurably significant in extension. A supine scan in these patients shows adequate foraminal dimensions and is reported as normal or mildly narrowed. The position-specific compression is missed entirely.
Who Should Consider a Flexion MRI After a Normal Supine Scan
For chronic pain patients with normal supine scans, the decision to pursue positional imaging often comes after months or years of being told that the imaging does not explain their symptoms. This is a population for whom a flexion and extension study frequently provides the first genuinely diagnostic result.
The specific clinical presentations that most warrant positional follow-up imaging include patients with symptoms that are clearly better lying down than standing or sitting, patients with leg symptoms that develop with walking and resolve with rest, patients who have a history of trauma with subsequent onset of spinal symptoms, and patients with known connective tissue disorders where ligamentous laxity is a systemic feature.
A full list of conditions that require positional imaging is useful for both patients and referring clinicians when evaluating whether a standard supine scan has been sufficient for a particular presentation.
Practical Considerations for Requesting a Flexion MRI
When requesting a positional or flexion MRI after a normal supine scan, the most useful information to include in the referral is the specific positions in which symptoms are provoked, the nature of the symptoms (pain, neurological, or both), and any prior imaging for comparison. The imaging centre can then select the positions most likely to reproduce the clinical scenario and maximise the diagnostic value of the study.
It is also worth noting that the interpretation of a positional study is more nuanced than a standard supine scan. Measurements need to be compared between positions, and the clinical significance of findings depends on the degree of positional change rather than on absolute values at a single time point. An experienced reading provider who is familiar with positional spine imaging adds significant value to the final report.
Frequently Asked Questions
If my supine MRI was normal, will insurance cover a flexion MRI?
Coverage for positional and flexion-extension MRI varies significantly by insurer and by the clinical justification provided. Some insurers cover these studies when there is documented symptom provocation in specific positions and a clinical rationale for why the supine scan was insufficient. Self-pay options are available at specialised upright imaging centres for patients whose coverage does not extend to these studies.
Can a flexion MRI be performed in a regular closed scanner?
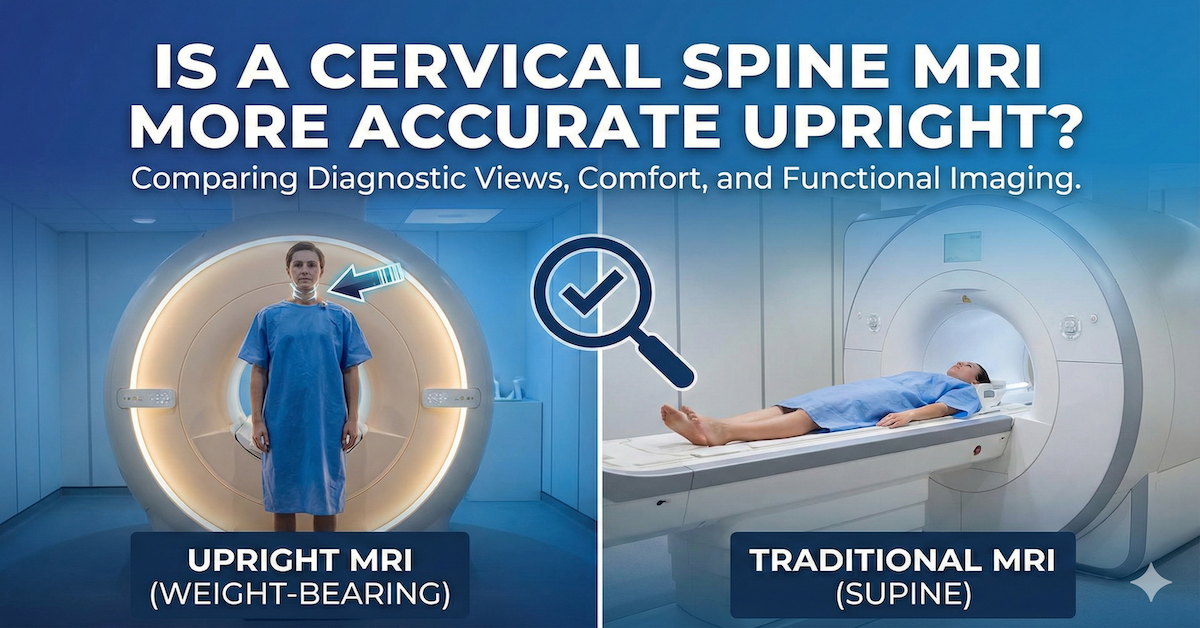
A true positional flexion MRI, with the patient in the flexed position under load, requires an open upright system that can accommodate the patient in a non-supine posture. A conventional closed bore scanner can image a patient lying in a slightly flexed position, which provides some additional information, but this is not equivalent to imaging the patient seated or standing with the spine under gravitational load in the flexed position.
How much more does a flexion MRI reveal compared to a standard scan?
In patients with position-dependent symptoms, studies comparing supine and upright or dynamic MRI have documented clinically significant additional findings in a meaningful proportion of cases. The yield is highest in patients with symptoms that are specifically provoked by position and lowest in patients with constant symptoms regardless of position.
Will my doctor need to see me again after reviewing the flexion MRI results?
Yes. A flexion MRI that reveals new findings needs to be interpreted in the context of the clinical picture, and the treating physician will need to discuss what the imaging means for the diagnosis and treatment plan. Some findings may simply confirm a clinical suspicion. Others may significantly change the direction of care.
What should I tell the imaging centre when requesting a flexion study?
Describe clearly which positions make your symptoms worse and which make them better. Note whether symptoms are provoked by standing, walking, forward bending, or extension. The more specifically you can describe your symptom provocation pattern, the more precisely the imaging team can position you to capture the most diagnostically relevant views.
The Bottom Line
A normal supine MRI is useful, but it is not the final word on whether structural spinal pathology is present. For patients whose symptoms are position-dependent and whose supine scan has not provided a diagnosis, a flexion MRI is often the next most informative step and frequently provides the structural explanation that has been missing.
Upright MRI of Deerfield performs flexion, extension, and full positional spine imaging as part of its standard approach to spinal assessment. If a supine scan has not explained your symptoms, reaching out for a consultation is a practical way to understand whether positional imaging would add the missing information.
SHARE THIS POST:
Leave a Comment:

The World's Most Patient-Friendly MRI. A comfortable, stress-free, and completely reliable MRI scan. We offer patients an open, upright, standup MRI experience that helps those who are claustrophobic and stress being in a confined area. Upright MRI of Deerfield is recognized as the world leader in open MRI innovation,
Our Recent Post








READ PATIENT TESTIMONIALS
Upright MRI of Deerfield.
Susan D.,
Highland Park, 39
I am going to tell everyone about your office! This was a great experience after I panicked in other MRI machines and had to leave. Thank you so much.

Judith B.,
Milwaukee, 61
I suffer from vertigo and other MRIs do not work. This was wonderful…absolutely NO discomfort at all. The MRI was so fast…I wanted to stay and watch the movie! Mumtaz was great. His humor really put me at ease. I’ve already recommended Upright MRI to friends.
Delores P.,
Glencoe, 55
Everything is so nice and professional with your place. I have been there a couple of times. My husband and I would not go anywhere else.

