
Can a Dynamic Spine MRI Help With Surgical Planning?
Spinal surgery is one of the more consequential decisions a patient and surgeon make together. The stakes are high, the recovery is significant, and the outcome depends heavily on whether the imaging used to plan the procedure accurately reflects what is actually happening in the spine under real-world conditions. The concern that has grown among experienced spine surgeons and imaging specialists is that conventional supine MRI, performed while the patient lies still in a closed scanner, may not be showing the full picture of what the spine is doing when the patient is actually upright, moving, and bearing weight.
Dynamic spine MRI addresses this limitation directly. By imaging the spine in multiple positions, including flexion, extension, and under the effect of gravity while seated or standing, it captures the structural behaviour of the spine across the range of positions in which symptoms actually occur. For surgeons planning a procedure, this additional information can change both the nature and the extent of the intervention being considered.
Quick Answer: Yes, a dynamic spine MRI can significantly improve surgical planning by revealing positional instability, dynamic compression, and movement-dependent pathology that a static supine scan does not show. When a surgeon bases a procedure on supine imaging that misses a segment of instability or a load-dependent stenosis, the surgical plan may be incomplete. Dynamic imaging adds the positional context that aligns the surgical target with the patient's actual functional anatomy.

What Dynamic Spine MRI Actually Captures
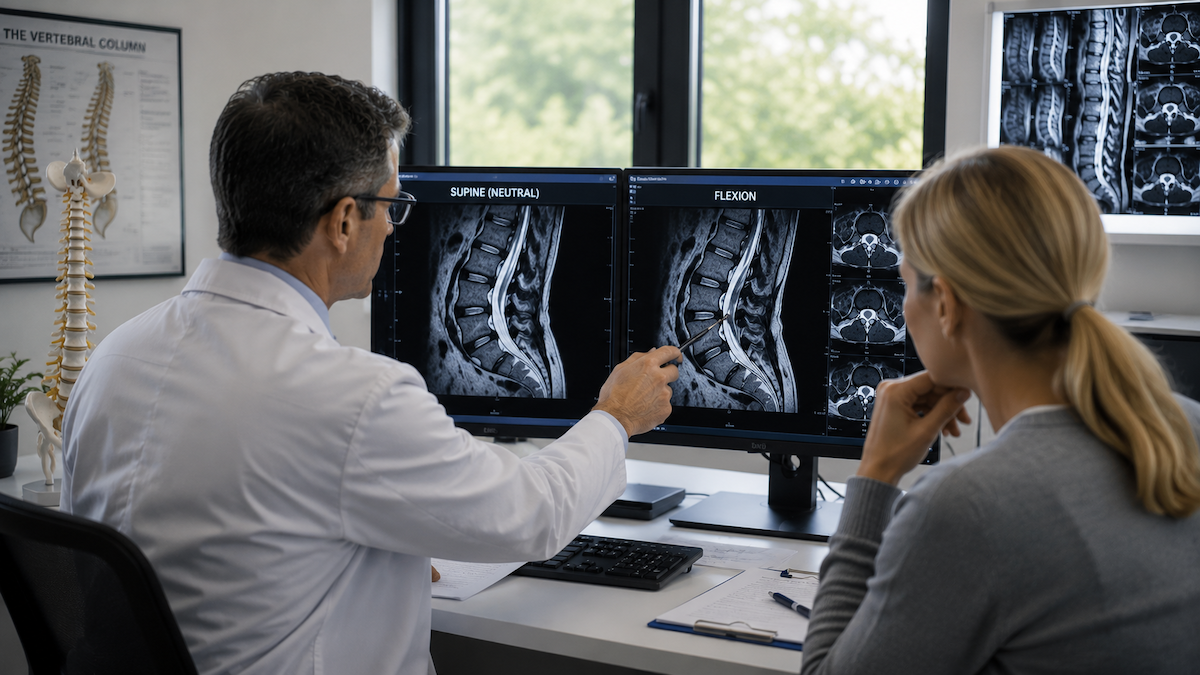
A dynamic spine MRI is not a single scan taken in one position. It captures the spine in at least two positions, typically flexion and extension, and often in the neutral upright and weight-bearing position as well. Each position reveals how the individual segments of the spine behave relative to each other under different loads and movements.
Ligamentous laxity, which allows adjacent vertebrae to shift beyond normal limits when the spine flexes or extends, is one of the most clinically significant findings that dynamic imaging reveals. This abnormal movement, called segmental instability, is often invisible on a neutral supine scan because the spine is not being stressed. When present, it is a directly relevant surgical finding: an unstable segment may require fusion or stabilisation that the surgeon would not have planned for based on static imaging alone.
The information that flexion and extension imaging reveals about dynamic instability is particularly relevant in the planning of fusion procedures, where identifying all unstable levels before the operation prevents the complication of fusing adjacent to a segment that will itself require stabilisation in the future.
How Load Changes What the Imaging Shows
When a patient lies in a supine scanner, the spine is offloaded. The intervertebral discs are decompressed, the foramina are at their widest, and the facet joints are at rest. The anatomy looks its best. A supine scan misses positional changes that occur when the patient stands up and the gravitational load is restored.
Under gravitational load, disc height can reduce, foraminal area narrows, and ligamentum flavum buckles into the spinal canal. These changes can produce nerve compression that is simply not present in the supine position. Weight-bearing spine imaging documents this load-dependent stenosis in real time, giving the surgeon a picture of what the nerve is actually experiencing when the patient is on their feet.
This distinction between positional and static pathology is directly relevant to surgical decision-making. A decompression procedure planned around supine imaging may address the anatomy as it appears at rest while leaving untouched the load-dependent compression that is actually responsible for the patient's symptoms. The dynamic scan aligns the surgical target with the functional problem rather than the resting anatomy.
The Cervical Spine: Where Dynamic Imaging Changes Plans Most Significantly
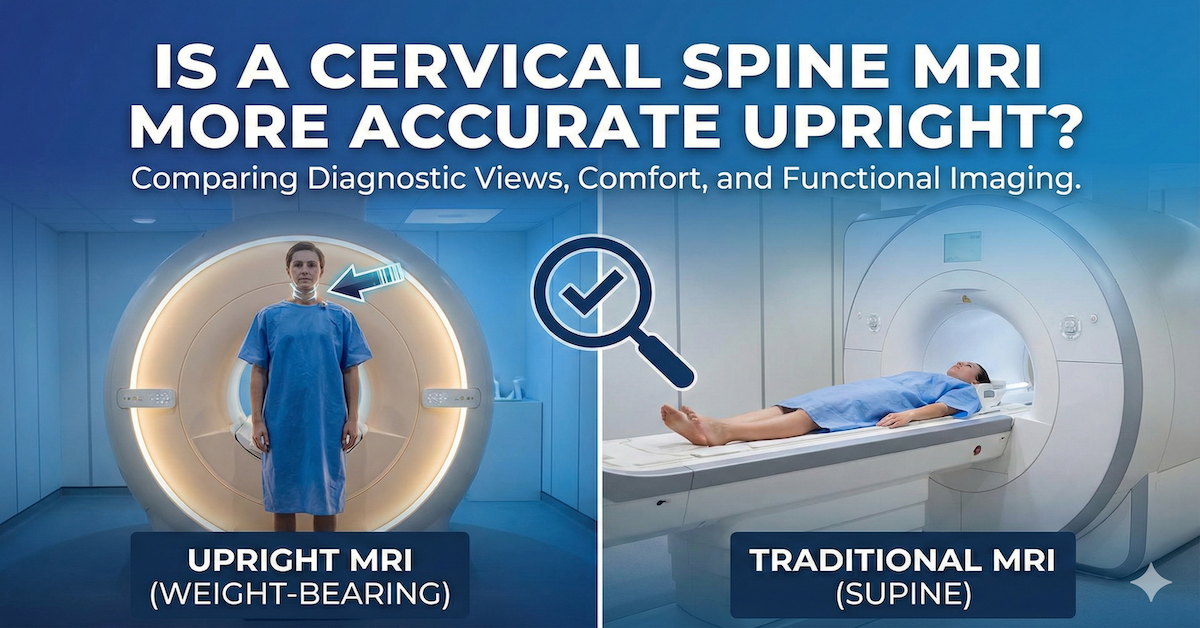
In the cervical spine, the consequences of positional instability can be particularly serious, and cervical spine imaging in the upright position consistently demonstrates findings that have direct bearing on whether surgical stabilisation is recommended, the number of levels that need to be addressed, and which surgical approach is most appropriate.
Patients with cervical instability often describe symptoms that worsen in specific head positions and improve when lying down. When their supine scan is normal or minimally abnormal, their symptoms may be dismissed as non-structural. Dynamic upright imaging in the positions that provoke their symptoms can demonstrate cord compression or canal compromise that was completely absent on the resting scan. This changes both the diagnosis and the surgical conversation entirely.
For patients with conditions such as Ehlers-Danlos syndrome, cranio-cervical instability, or significant cervical disc disease, the gap between supine and positional imaging can be the difference between a scan that directs surgery accurately and one that directs it toward the wrong target.
The Lumbar Spine: Dynamic Findings That Alter the Surgical Plan
In the lumbar region, lumbar flexion MRI reveals hidden compression of the thecal sac and nerve roots that is not apparent on a neutral supine scan, particularly in patients with ligamentum flavum hypertrophy, which buckling further during flexion as the posterior ligamentous structures shorten.
Anterolisthesis and retrolisthesis, the forward and backward slippage of one vertebra on another, can be minimal on a neutral scan and dramatically more apparent on dynamic imaging. A patient whose supine scan shows a 3mm slip may show a 7mm slip in extension, which completely changes the clinical significance of that finding and the surgical planning for that level.
Spondylolisthesis in particular benefits from dynamic imaging before surgical planning. When a slip is mobile rather than fixed, the surgeon needs to know this before deciding whether reduction is possible, whether it should be attempted, and whether additional fixation will be required to maintain the corrected position after surgery.
For Physicians: What Dynamic Imaging Adds to the Referral Picture
Referring physicians who are considering a spinal surgery consultation for a patient with ongoing symptoms despite apparently normal or mildly abnormal supine imaging should consider whether upright MRI for flexion and extension imaging would provide the additional positional context that changes the clinical picture.
The physician referral resource at Upright MRI of Deerfield outlines the specific imaging protocols available, how to request positional and dynamic studies, and how the reports are structured to provide maximum clinical utility for surgical consultants.
For patients scheduled for back and spine MRI services who have symptoms that are clearly worse in specific positions or under load, requesting dynamic sequences at the time of referral ensures the scan will capture the clinically relevant positional information rather than just the resting anatomy.
What Surgeons Look for in a Dynamic MRI Report
A well-structured dynamic spine MRI report for surgical planning purposes should document the range of motion at each level, any abnormal translational movement that exceeds normal limits, the change in foraminal and canal dimensions between positions, and the position at which maximum compression occurs. Comparative measurements between positions are more informative than single-position measurements alone.
When the report identifies a level as showing significant dynamic instability or position-dependent compression, this finding should be correlated with the patient's symptom provocation pattern. The most useful reports are those where the imaging positions were selected to match the positions in which the patient experiences their worst symptoms, so the imaging and the clinical story align directly.
Frequently Asked Questions
Can a dynamic MRI replace a surgical CT scan for planning purposes?
Not typically, because CT provides superior bony detail that MRI cannot match, particularly for evaluating facet joint anatomy, pedicle dimensions for screw placement, and cortical bone integrity. Dynamic MRI and CT are complementary rather than interchangeable in surgical planning, with dynamic MRI providing the functional and soft tissue dimension and CT providing the structural bone detail.
Will my surgeon specifically request a dynamic MRI, or do I need to ask?
Some surgeons routinely request dynamic studies as part of their pre-surgical workup. Others may not be familiar with the availability of upright positional imaging or may default to conventional supine protocols. Patients who have position-dependent symptoms or who have had normal supine scans despite significant symptoms can specifically ask their surgeon whether dynamic or positional imaging would add useful information before a surgical decision is made.
Is a dynamic spine MRI more expensive than a standard scan?
The pricing depends on the facility and the specific protocol. At centres that offer upright positional imaging, the additional positional sequences typically add to the base scan cost. For patients considering spinal surgery, the cost of a more complete pre-operative imaging study is generally modest relative to the cost and consequences of a surgical intervention.
Are there spine conditions that do not benefit from dynamic imaging?
Fixed structural changes, such as a large calcified disc herniation or post-surgical scar tissue that does not change with position, may not show significantly different findings on dynamic versus static imaging. Dynamic imaging adds most value when the pathology is positional, ligamentous, or load-dependent. A pre-scan consultation can help determine whether dynamic sequences are warranted for a specific situation.
Can dynamic spine imaging be performed in both the cervical and lumbar regions in one visit?
Yes. An upright positional MRI system can perform multiple spinal regions in different positions within a single session. If both cervical and lumbar pathology is being evaluated for surgical planning, both regions can be imaged in flexion, extension, and neutral in one visit, which is considerably more efficient than multiple appointments.
The Bottom Line
Dynamic spine MRI provides the positional context that static supine imaging cannot offer, and for spinal surgical planning, that context can change the procedure being recommended, the levels being addressed, and the surgical approach being used. Patients whose symptoms are clearly position-dependent, and surgeons planning interventions based on supine imaging alone, both benefit from the additional information it provides.
Upright MRI of Deerfield specialises in exactly this type of positional and dynamic spine imaging. If you or your surgeon are working toward a surgical decision and want the most complete pre-operative imaging picture available, a consultation or referral is a practical next step.
SHARE THIS POST:
Leave a Comment:

The World's Most Patient-Friendly MRI. A comfortable, stress-free, and completely reliable MRI scan. We offer patients an open, upright, standup MRI experience that helps those who are claustrophobic and stress being in a confined area. Upright MRI of Deerfield is recognized as the world leader in open MRI innovation,
Our Recent Post







READ PATIENT TESTIMONIALS
Upright MRI of Deerfield.
Susan D.,
Highland Park, 39
I am going to tell everyone about your office! This was a great experience after I panicked in other MRI machines and had to leave. Thank you so much.

Judith B.,
Milwaukee, 61
I suffer from vertigo and other MRIs do not work. This was wonderful…absolutely NO discomfort at all. The MRI was so fast…I wanted to stay and watch the movie! Mumtaz was great. His humor really put me at ease. I’ve already recommended Upright MRI to friends.
Delores P.,
Glencoe, 55
Everything is so nice and professional with your place. I have been there a couple of times. My husband and I would not go anywhere else.

